
Definition
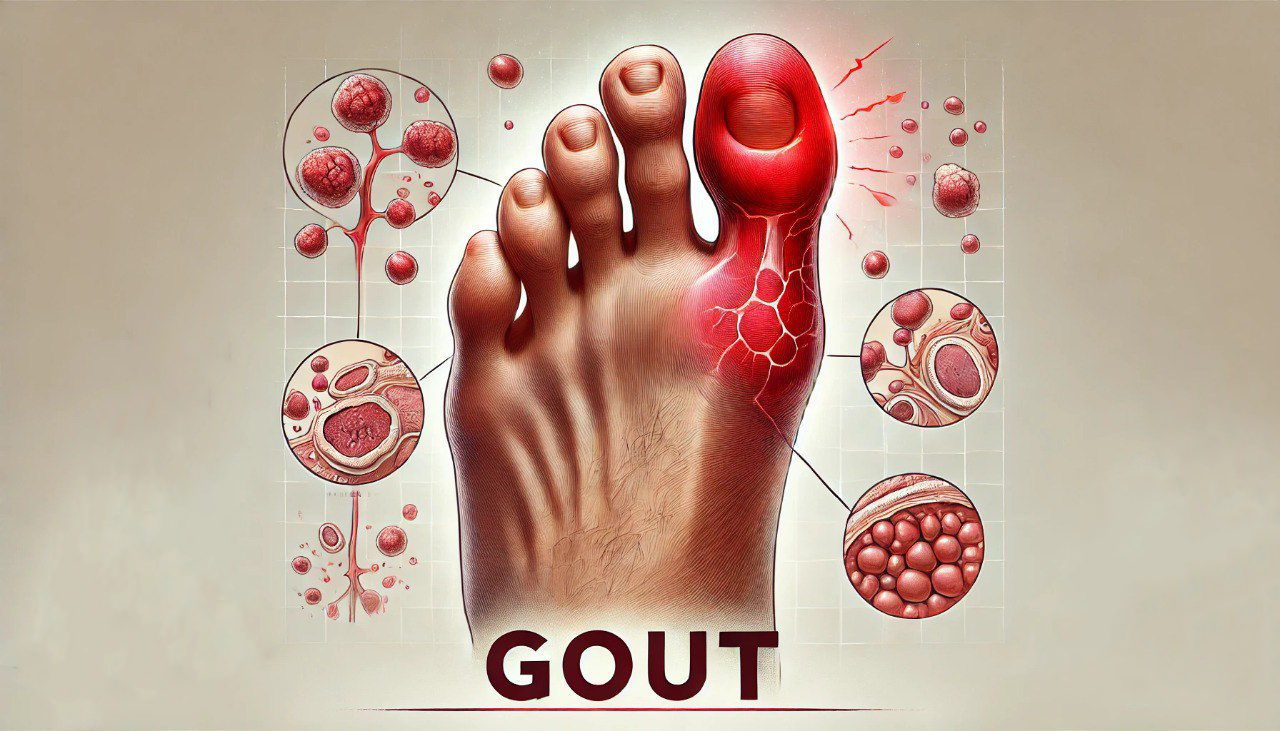
Gout is a crystal-induced arthritis. It is characterized by recurrent attacks of acute arthritis, with deposition of sodium urate crystals in tissues due to increased uric acid in the blood.
Gouty arthritis is a disease caused by purine metabolism disorder, belonging to a group of metabolic disorders.
Causes
Primary gout
- For unknown reasons, a diet high in purines such as liver, kidney, shrimp, crab, egg yolks, and mushrooms aggravates the disease.
- Occurs in 95% of men; the typical age is 30-60.
Secondary gout
A rare case is due to genetic disorders (genetic causes).
In addition, it can be due to increased uric acid production, creased uric acid excretion, or both, specifically:
- Renal failure in particular, and diseases that generally reduce uric acid clearance by the glomerulus.
- Blood diseases: acute leukemia.
- Use of diuretics such as Furosemide, Thiazide, Acetazolamide.
- Use cell inhibitors to treat malignant diseases and anti-tuberculosis drugs (ethambutol, pyrazinamide).
Risk factors for the disease are high blood pressure, obesity and metabolic syndrome, hyperinsulinemia and insulin resistance, and heavy alcohol consumption.
Symptom
The first acute gout attack usually occurs between the ages of 35 and 55, rarely before 25 or after 65. In women, it seldom happens before menopause; in men, the younger the age, the more severe the disease.

- Acute gout attack: Appears suddenly at night, and the patient wakes up because of pain in the joints. Usually, the metatarsal joint – big toe (60 – 70%): the joint is swollen, red, edematous, shiny, hot, and severe pain, and increasing light contact is also excruciating, changing order: foot, ankle, knee, hand, wrist, elbow, rarely in the hip, shoulder, spine. At first, only one joint is inflamed, then many joints can be inflamed.
- In addition to the joint, the bursa, tendons, and joint capsule can also be damaged
- Signs of inflammation can last for many days, usually 5-7 days, then the signs of inflammation gradually decrease less pain, swelling, and redness. After the attack, the joint returns to entirely normal.
- Acute gout attacks are easy to recur; the interval can be close but very far, sometimes > ten years.
- Urate deposition causes the formation of tophi under the skin and causes chronic urate arthritis.
- Tophi: It often manifests slowly, decades after the first gout attack, but sometimes earlier. Once it appears, it can quickly increase in number and mass and ulcerate.
- Urate deposits scattered in the renal interstitium, renal pelvis, and ureter, causing urate kidney stones and kidney damage.
Diagnosis
Bennet and Wood criteria (1968): sensitivity of 70%, specificity of 82.7% is the most widely applied in Vietnam because it is easy to remember and suitable for the lack of testing conditions.
ILAR and Omeract criteria in 2000: Sensitivity 70%, specificity 78.8%.
Necessary paraclinical tests:
- Increased blood uric acid > 420 µmol/l; about 40% of patients have acute gout but normal blood uric acid.
- 24-hour urinary uric acid quantification: if uric acid increases in urine, it can easily cause kidney stones, and uric acid excretion-increasing drugs are not indicated.
- Joint fluid test: look for urate crystals in joint fluid.
- Other tests include increased erythrocyte sedimentation rate and normal or increased CRP.
- Joint X-ray: average in the early stages; if late, bone defects in the form of cavities at the bone ends, narrowed joint spaces, and bone spurs can be seen.
Differential diagnosis
- Arthritis due to the deposition of other crystals (calcium pyrophosphate dihydrate) or pseudogout.
- Infectious arthritis.
- Rheumatoid arthritis.
- Reactive arthritis.
- Other pathologies: cellulitis, peripheral vascular disease.
Treatment
Gouty arthritis is very easy to relapse and brings severe symptoms and complications to the patient if not treated and controlled strictly.
General principles
- Treatment of arthritis in acute gout.
- Prevention of gout recurrence, urate deposition in tissues, and prevention of complications through treatment of hyperuricemia syndrome.
Non-drug treatment
- Avoid foods high in purines, such as animal organs, meat, fish, shrimp, and crab. You can eat eggs and fruits. Eat no more than 150g of meat/24 hours.
- Do not drink alcohol, need to lose weight, and exercise regularly.
- Drink plenty of water, about 2-4 liters/24 hours, especially alkaline mineral water or 14‰ alkaline water.
- Avoid drugs that increase uric acid in the blood, and avoid factors that trigger acute gout attacks, such as stress and trauma.
Drug treatment
- Anti-inflammatory drugs: Colchicine usually responds well to gout, reducing pain and swelling in 1-2 days, but it is necessary to pay attention to the side effects of the drug.
- Non-steroidal anti-inflammatory drugs: Ketoprofen, Piroxicam, Diclofenac, Celecoxib.
- Systemic corticosteroids are indicated when the above drugs are ineffective or contraindicated and should be limited and used for a short time.
- Uric acid synthesis inhibitors: Allopurinol.
- Uric acid excretion-increasing drugs: Probenecid, this group requires urine uric acid testing.
Surgical treatment
- Tophi removal surgery is indicated in cases of gout with ulcer complications, tophi infection, or large tophi, affecting movement or for aesthetic reasons. When performing surgery, it is essential to use colchicine to avoid triggering an acute gout attack. It is necessary to combine drugs to lower blood uric acid.
Prevention
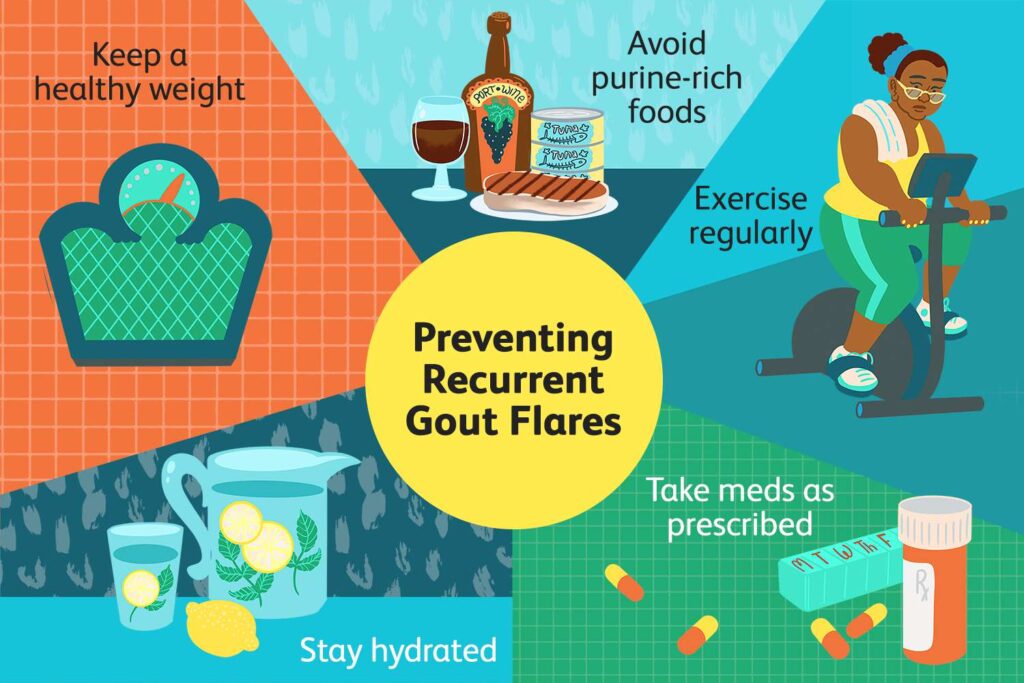
- A reasonable lifestyle and reduced intake of foods rich in purines and fats.
- Exercise.
- Treat healthy diseases that cause secondary gout, such as kidney failure, drugs, and metabolic diseases.